Neuromodulation & Brain Training
CLICK TO HEAR AN AI GENERATED DISCUSSION OF NEUROMODULATION/NEUROFEEDBACK/BIOFEEDBACK DISCUSSED ON THIS PAGE:
Please note, while there is burgeoning evidence (see: https://isnr.org/isnr-comprehensive-bibliography and https:// aapb.org/Disorders and https://www.vielight.com/research/ and https://alpha-stim.com/research-and-reports/) for neurofeedback, biofeedback, and other neuromodulation therapies for the treatment of various neurological and psychological disorders and to improve stress and performance, for specific disorders there are treatments that have more research supporting them (see: https://www.apa.org/practice/guidelines/evidence-based-statement). For ex? ample, for most anxiety disorders (including OCD and PTSD) exposure-based psychotherapies (e.g., CBT, ACT, Pro? longed Exposure etc.) have the most supporting evidence. Similarly, there is significant research supporting the use of medications (e.g., SSRI antidepressants) and various forms of psychological therapies (e.g., CBT, ACT, Behavioural Activation, etc.) for the treatment of anxiety and depression. In addition, the most evidence-based treatment of per? sonality disorders such as Borderline Personality Disorder (BPD), is Dialectical Behaviour Therapy (DBT). Therefore, if you have one of these disorders, we recommend you try these other therapies before neurofeedback, biofeedback, and other neuromodulation therapies. Similarly, most concussions improve on their own with time and slow re-activ? ation of your previous lifestyle and thus we generally do not recommend our neurofeedback, biofeedback, and other neuromodulation therapies in the early stages of concussion recovery.
• https://isnr.org/isnr-comprehensive-bibliograph
• https://aapb.org/Disorders
• https://www.vielight.com/research/
• https://alpha-stim.com/research-and-reports/
Hear Dr. Friesen discuss neurofeedback, biofeedback, brain mapping, and other forms for neuromodulation on Mindhacker’s Radio: #04 Dr. Chris Friesen: Upgrading and Biohacking the Mind with Neurofeedback, HRV Training, Photobiomodulation, and more! (or on iTunes Sept 11, 2019)
While I don’t necessarily agree with all of what Dr. Daniel Amen thinks and recommends, his Ted Talk on the importance and power of brain imaging is a good starting point for learning about your brain:
Dr. Normal Doidge helped popularize the concept of neuroplasticity or how the brain can change with experience and various non-invasive treatments. These were popularized in his best-selling books:
The Brain That Changes Itself The Brain’s Way of Healing:
![]()
To learn more, watch the CBC’s The Nature of Things with David Suzuki documentaries below:
WHAT IS NEUROFEEDBACK?
 Neurofeedback (also known as Neurotherapy or EEG Biofeedback), is a type of biofeedback that uses real-time displays of brain activity, to teach self-regulation of brain function. Sensors are placed on the head to measure brain activity at particular sites, with this brain activity fed back to the client via a computer screen. The client learns to increase or decrease brain activity to improve health and performance. In other words, neurofeedback teaches you to modify your brain activity. Over time, these changes may endure without continued use of neurofeedback (adapted from The International Society for Neurofeedback and Research www.isnr.org).
Neurofeedback (also known as Neurotherapy or EEG Biofeedback), is a type of biofeedback that uses real-time displays of brain activity, to teach self-regulation of brain function. Sensors are placed on the head to measure brain activity at particular sites, with this brain activity fed back to the client via a computer screen. The client learns to increase or decrease brain activity to improve health and performance. In other words, neurofeedback teaches you to modify your brain activity. Over time, these changes may endure without continued use of neurofeedback (adapted from The International Society for Neurofeedback and Research www.isnr.org).
To learn more about neurofeedback, please read Dr. D. Corydon Hammond’s article What Is Neurofeedback: An Update by clicking HERE.
WHAT IS BIOFEEDBACK?
Biofeedback is a similar process that enables a client to learn how to change physiological activity for the purposes of improving health and performance. Precise instruments measure physiological activity such as heart function (e.g., Heart Rate Variability or HRV), breathing, muscle activity, skin conductance (i.e., sweating), and skin temperature. These instruments quickly “feed back” information to the client. The presentation of this information — often in conjunction with changes in thinking, emotions, and behaviour — supports desired physiological changes. Over time, these changes can endure without continued use of an instrument (adapted from The International Society for Neurofeedback and Research www.isnr.org).
WHAT CAN NEUROFEEDBACK & BIOFEEDBACK HELP WITH?
Neurofeedback and Biofeedback are used to treat ADHD, anxiety, depression, stress, epilepsy, headaches, TBI, strokes, and to help with optimal performance for those who want to perform at their best such as students, entrepreneurs, executives, and athletes.
The American Association of Applied Psychophysiology and Biofeedback (AAPB) and The International Society for Neurofeedback and Research (ISNR) have created a list of different levels of efficacy of neurofeedback and biofeedback for various applications. For some applications, neurofeedback is an accepted treatment, while for other conditions it shows promise, or should it still be considered to be an experimental method.
The AAPB has developed the following criteria for setting the level of evidence for efficacy (Moss and Gunkelman 2002, LaVaque et al 2002): It is very similar to the rating schemes developed by other organizations such as the American Psychological Association. Please note that the efficacy ratings made based on these criteria are from formal studies.
Level 1: Not empirically supported: Supported only by anecdotal reports and/or case studies in non-peer-reviewed venues.
Level 2: Possibly Efficacious: At least one study of sufficient statistical power with well-identified outcome measures, but lacking randomized assignment to a control condition internal to the study.
Level 3: Probably Efficacious: Multiple observational studies, clinical studies, waitlist controlled studies, and within-subject and intrasubject replication studies that demonstrate efficacy.
Level 4: Efficacious:
a.) In a comparison with a no-treatment control group, alternative treatment group, or sham (placebo) control utilizing randomized assignment, the investigational treatment is shown to be statistically significantly superior to the control condition or the investigational treatment is equivalent to a treatment of established efficacy in a study with sufficient power to detect moderate differences, and
b.) The studies have been conducted with a population treated for a specific problem, for whom inclusion criteria are delineated in a reliable, operationally defined manner, and
c.) The study used valid and clearly specified outcome measures related to the problem being treated and
d.) The data are subjected to appropriate data analysis, and
e.) The diagnostic and treatment variables and procedures are clearly defined in a manner that permits replication of the study by independent researchers, and
f.) The superiority or equivalence of the investigational treatment has been shown in at least two independent research settings.
Level 5: Efficacious and specific: The investigational treatment has been shown to be statistically superior to credible sham therapy, pill, or alternative bona fide treatment in at least two independent research settings.
Efficacy Ratings for Neurofeedback & Biofeedback-Based Treatments:
The following is adapted from Tan, Shaffer, Lyle, & Two (2016) Evidence-Based Practice in Biofeedback and Neurofeedback. Association for Applied Psychophysiology and Biofeedback. Colorado Springs, CO.
*Only included are conditions treated by Niagara Neuropsychology staff.
Efficacious and specific (Fifth & highest level):
- Attention-Deficit/Hyperactivity Disorder (ADD/ADHD)
Efficacious (Fourth Level) :
- Anxiety
- Depressive Disorders
- Chronic Pain
- Epilepsy/Seizures
- Irritable Bowel Syndrome (IBS)
- Headaches/Migraines
- Hypertension
- Raynaud’s Disease
Probably efficacious (Third level):
- Traumatic Brain Injury/Concussion
- Posttraumatic Stress Disorder/PTSD
- Performance Enhancement
- Insomnia
- Chemo Brain
- Fibromyalgia/Chronic Fatigue Syndrome
Possibly Efficacious (Second level):
- Stroke
Dr. Andrew Hill from the Peak Brain Institute provides a good summary of some of the key studies on neurofeedback. You can see this by clicking HERE or by clicking the links below:
ADHD & Learning Disabilities
Anxiety
Autism & Asperger’s
Chronic Fatigue
Cognitive Enhancement & Decline
Depression
Developmental Disabilities
Migraines
Post-Traumatic Stress Disorder
Seizures
Sleep
Substance Use Disorders
Traumatic Brain Injury
Applied Psychophysiology Education (APEd) has a comprehensive list of abstracts for neurofeedback research that you can access HERE.
To hear Dr. Bessel van der Kolk (author of The Body Keeps Score) discuss neurofeedback for trauma and PTSD, click the short video below:
Similarly, the International Society for Neuroregulation & Research (ISNR.org) regularly updates a comprehensive bibliography of neurofeedback research studies that can be accessed HERE.
Below is one girl’s experience trying to improve her sleep and focus with a brief trial of neurofeedback:
Below is Maggie’s Story, a short video about a young girl whose seizures were successfully reduced with neurofeedback. For those interested in the research, click HERE, HERE, and HERE.
To learn more watch Dr. Velkoff from the Drake Institute discuss ADHD on Lifestyle Magazine HERE:
HOW LONG DOES NEUROFEEDBACK & BIOFEEDBACK TRAINING TAKE?
Neurofeedback training typically requires 20 or more sessions, usually held twice or more weekly. Biofeedback training typically takes much less but requires home practice.
NEUROFEEDBACK VIDEOS:
Here is a video on how neurofeedback can help with depression:
This video is from CNN on how neurofeedback can help with ADHD and anxiety:
To hear a great podcast where Dr. Andrew Hill discusses neurofeedback, click below:
Learn some of the basic science behind neurofeedback here:
To learn more about the latest on how we now assess and treat concussions from my colleague, Dr. Robert Conder (former Carolina Hurricanes team neuropsychologist), watch the videos below:
To learn more about concussions, more significant TBIs, and how to treat them with neurofeedback and biofeedback, listen to Dr. Friesen’s interview on the Heal Better Fast podcast with Dr. Michael Pound by clicking HERE.
Dr. Friesen is board certified in Neurofeedback through the Biofeedback International Certification Alliance (BCIA) and we are offering biofeedback, neurofeedback, and other neuromodulation treatments.
Excellent book on the history, research, and potential of neurofeedback.
 QUANTITATIVE EEG (qEEG) or “BRAIN MAPPING”
QUANTITATIVE EEG (qEEG) or “BRAIN MAPPING”
Electroencephalography (EEG) is the measurement of electrical patterns at the surface of the scalp which reflect cortical activity, and are commonly referred to as “brainwaves”. Quantitative EEG (qEEG) is the analysis of the digitized EEG, and in lay terms, this sometimes is also called “Brain Mapping”. The qEEG is an extension of the analysis of the visual EEG interpretation which may assist and even augment our understanding of the EEG and brain function.
Quantitative Electroencephalography (qEEG) is a procedure that processes the recorded EEG activity from a multi-electrode recording using a computer. The digital data is statistically analyzed, comparing values with “normative” database reference values. The processed EEG is commonly converted into color maps of brain functioning called “Brain Maps”.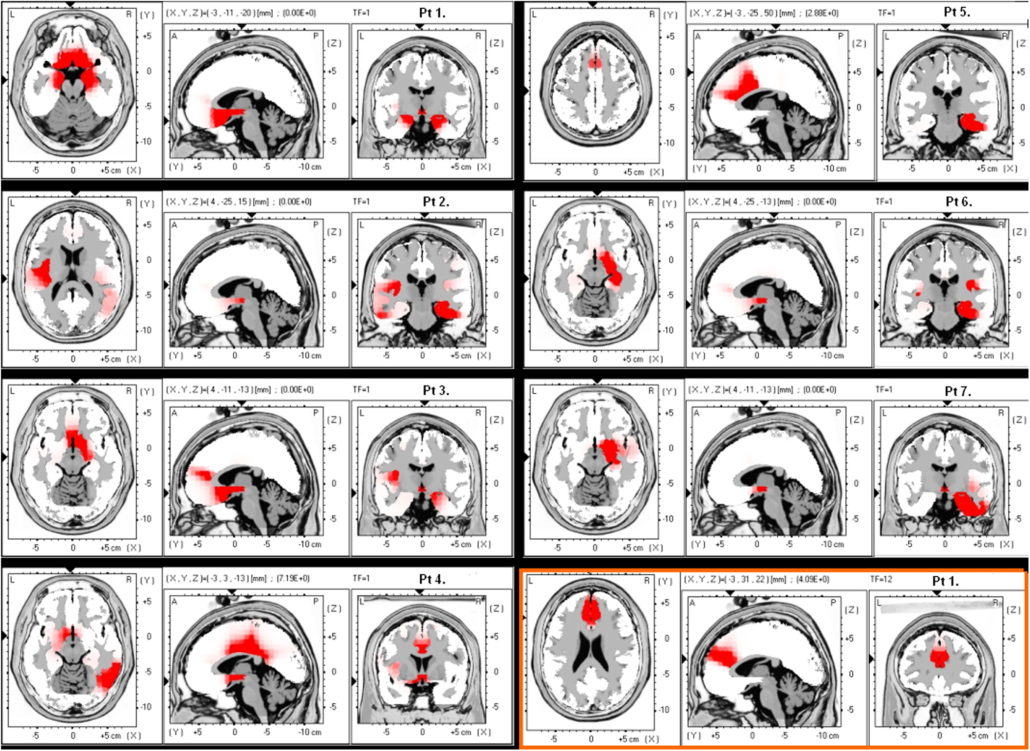
The EEG and the derived qEEG information can be interpreted and used by experts as a clinical tool to evaluate brain function and to track the changes in brain function due to various interventions such as neurofeedback or medication.
The use of advanced techniques such as Independent Component Analysis (ICA) and neuroimaging techniques such as Low-Resolution Electromagnetic Tomography (LORETA) can map the actual sources of the cortical rhythms. These advanced approaches are changing our understanding of the dynamics and function of the human brain.
Why do a qEEG for Neurofeedback?
 There are many in the field of neurofeedback who do not perform qEEGs prior to designing a clinical intervention. These people are currently practicing well within the standard of practice for this rapidly evolving field.
There are many in the field of neurofeedback who do not perform qEEGs prior to designing a clinical intervention. These people are currently practicing well within the standard of practice for this rapidly evolving field.
There is an increasing body of evidence that there is a positive treatment impact from the use of a qEEG and the resultant customized neurofeedback intervention.
Clinical applications of qEEG
The qEEG is used by those currently in a professional practice for the following clinical applications: evaluating effects of medications and predicting medication response, evaluating head traumas, assessment of cognitive and psychiatric changes, in neurofeedback, and in peak performance assessment and training as well as others.
Adapted from qeegsupport.com
OTHER NEUROMODULATION TREATMENTS
A number of other neuromodulation techniques offered at Niagara Neuropsychology include the Low Energy Neurofeedback System (LENS, HPN, LIP-tES), Cranial Electrotherapy Stimulation (CES), Transcranial Direct Current Stimulation (tDCS), and Transcranial Photobiomodulation.
The Low Energy Neurofeedback System (LENS), also known as High-Performance Neurofeedback (HPN), Microcurrent Neurofeedback, Direct Neurofeedback, and Low-Intensity Pulsed Transcranial Electrical Stimulation (LIP-tES), is rapidly gaining evidence to help those with numerous conditions including anxiety/depression, PTSD, pain, addictions, and various forms of central nervous system dysfunction (e.g., TBI/Concussions, cognitive impairment, ADHD, etc.). Preliminary research has found such treatment effective for those with TBI/Concussions. There is a strong research focus on TBI/Concussions and PTSD in former NFL players and returning veterans.
Here are some examples of the clinical research using LENS and related treatments:
- University of California summary of MEG study of HPN treatment of veterans with Mild TBI/Concussion & post-concussion syndrome: Click HERE and HERE
- Dr. Stephen Larsen’s article in the journal Biofeedback titled The Special Applicability of the LENS Form of Neurofeedback to TBI: Click HERE
- Multisite case series of retired NFL players with multiple concussions and post-concussion syndrome treated with Direct Neurofeedback: Click HERE
- Dr. Stephen Larsen’s clinical outcomes study using LENS on 100 patients in the Journal of Neurotherapy: Click HERE
- Dr. Corydon Hammond’s case study and qEEG analysis of a young woman with a severe TBI in the Journal of Neurotherapy: Click HERE
For a special issue of the Journal of Neurotherapy devoted to LENS, click HERE.
For a list of LENS references, click HERE.
Videos of patient experiences and other information on LENS and related treatments:
- Patient success stories: Click HERE and HERE
- NBC story about first responders getting treatment for PTSD: Click HERE
- ABC News stories on research and treatment with football players: Click HERE and HERE
- CBS News piece on former Denver Broncos players getting relief from LENS: Click HERE
- Former NFL players, Jessie Sapolu, Kermit Alexander, & Craig McEwen’s, experiences with repeated concussions and treatment with Direct Neurofeedback: Click HERE
- Former NFL players, Mark Robinson and Mark Cotney’s experiences with repeated concussions and treatment with HPN: Click HERE
- Former NFL player, Gerry Wunsch’s, experience with repeated concussions and treatment with HPN: Click HERE
- Segment on The Doctors TV show: Click HERE
- Young woman with Cerebral Palsy and a TBI treated with LENS: Click HERE
For further reading:
- Dr. Stephen Larsen’s book: The Healing Powers of Neurofeedback
- Dr. Stephen Larsen’s other book: The Neurofeedback Solution
See video below for a short documentary about a man who developed PTSD in a horrific helicopter crash who was successfully treated with LENS:
To hear one of the top neuromodulation (aka Electroceuticals) researchers (Vincent Clark, Ph.D.) discuss the research and potential of such modalities, click here:
Alpha-Stim AID
Briefly, Cranial Electrotherapy Stimulation (CES) utilizes extremely small levels of electrical stimulation across the head. It has been found to be efficacious for a number of difficulties including anxiety, depression, insomnia, and chronic pain. CES units are approved in the United States by the Federal Drug Administration (FDA) for the treatment of anxiety, depression, and insomnia. Click here and here to learn more. Click here for a list of references.
Evidence from published research suggests CES use activates particular groups of nerve cells that produce the neurotransmitters serotonin and acetylcholine which can affect the chemical activity of nerve cells that are both nearby and distant in the nervous system. By changing the electrical and chemical activity of certain nerve cells, CES devices like Alpha-Stim® (seen on the left) appear to amplify activity in some neurological systems and deactivate activity in others. This neurological ‘fine tuning’ occurs either as a result of or together with the production of a certain type of electrical activity pattern in the brain known as an alpha state. CES has been found increase alpha and decrease delta, theta, and beta waves on qEEG brain maps. This typically results in feeling calm, relaxed and focused. This appears to decrease stress effects, reduce agitation, stabilize mood, and regulate both sensations and perceptions of particular types of pain.
Adapted from Alpha-Stim.com
Here is a brief video of the use of CES in the British Health System in the treatment of Generalized Anxiety Disorder (GAD) and a 1-minute video from one of the manufactures of a CES device:
According to the Johns Hopkins School of Medicine, “tDCS is a non-invasive, painless brain stimulation treatment that uses direct electrical currents to stimulate specific parts of the brain. A constant, low-intensity current is passed through two electrodes placed over the head which modulates neuronal activity. There are two types of stimulation with tDCS: anodal and cathodal stimulation. Anodal stimulation acts to excite neuronal activity while cathodal stimulation inhibits or reduces neuronal activity.
Although tDCS is still an experimental form of brain stimulation, it potentially has several advantages over other brain stimulation techniques. It is cheap, non-invasive, painless and safe. It is also easy to administer and the equipment is easily portable. The most common side effect of tDCS is slight itching or tingling on the scalp.
Several studies suggest it may be a valuable tool for the treatment of neuropsychiatric conditions such as depression, anxiety, Parkinson’s disease, and chronic pain. Research has also demonstrated cognitive improvement in some patients undergoing tDCS. Currently, tDCS is not an FDA-approved treatment.”
tDCS involves the application of a constant, low current to the brain area of interest via electrodes on the head. It is believed to increase or decrease neural excitability (depending on the electrode configuration). tDCS is currently an experimental treatment for various conditions such as depression, anxiety, and brain injuries including strokes. Research to date suggests there are no serious side-effects or reported adverse events (click here for a recent review of adverse events). There is evidence that tDCS can improve psychological problems such as depression and possibly anxiety (click here, here and here). In addition, there is evidence that tDCS can improve cognitive performance in otherwise healthy subjects (click here and here) and possibly enhance cognitive functions in those with brain damage (click here). For a 2014 review of the research click here. For a 2016 review of the research, click here.

VieLight Neuro
Transcranial Photobiomodulation (aka Neurophotomodulation) or low-level light therapy (LLLT) involves the use of low-level near-infrared light to stimulate neuronal mitochondria and cellular events. These lights are applied to the patient’s head for therapeutic purposes such as recovery from neurological disorder or damage. Light in the red and near-infrared regions of the electromagnetic spectrum are used because of their ability to penetrate the scalp, skull, and brain. Studies have been performed to assess the safety and effectiveness of transcranial light therapy in conditions such as depression, stroke, traumatic brain injury (TBI), and neurodegenerative conditions.
VieLight Neuro
For a review of the research, click here (general review), here , here, here , here, here, and here (Alzheimer’s and Parkinson’s disease), here , here (TBI), here (mild TBI/concussions) here, here (improved cognitive and mood in healthy subjects), here (reduction in depression in patients with Major Depressive Disorder) and here (references).
The first study to report significant cognitive improvement in dementia participants following brain photobiomodulation treatments was presented at the Alzheimer’s Association International Conference in Toronto in July 2016. To see the abstract, click here. To see the poster, click here. To see a related news clip click here.
Due to the fact that only recently have researchers started to use transcranial photobiomodulation in the treatment of brain disorders and, although transcranial photobiomodulation is considered safe, at this point in time it is considered experimental and thus no medical claims can be made.
Here is a video from the University of Utah of concussion and TBI patients & their families discussing the positive outcomes they experienced using the Vielight Neuro Transcranial Photobiomodulation (tPBM) unit. We’ve been offering this at our clinic for a number of years.
This is an article about a former football player and boxer who benefited from tPBM treatment that we offer:
Boxing and football put him in a fog, light therapy gave him his life back
A study of collision athletes at the University of Utah department of neurology indicates an infrared light therapy called transcranial photobiomodulation helps relieve the symptoms of brain trauma
Audio-Visual Entrainment (AVE)* is a technique that utilizes pulses of light and sound at specific frequencies to gently and safely guide the brain into various brain wave patterns. By altering your brain wave frequencies, you have the ability to boost your mood, improve sleep patterns, sharpen your mind and increase your level of relaxation.

AVE is capable of producing situationally appropriate brain wave frequencies through the process of entrainment (the tendency of physiological processes to mirror environmental stimuli). AVE also increases cerebral blood flow (blood flow in the brain) and increases the metabolization of glucose in the brain for improved functioning of the neurons. The combined outcome of these processes is improved mental performance. It is an effective, inexpensive alternative therapy for many disorders such as anxiety, Attention Deficit Disorder (ADD), Seasonal Affective Disorder (SAD), PTSD, Fibromyalgia and chronic pain. AVE devices are also used successfully to boost physical performance for athletes, academic performance for students and cognitive performance for seniors.
For a comprehensive review of the psychological effects of AVE click HERE.
An important objective of entrainment is to produce a dissociative state, which is a meditation-like state of deep relaxation. It is the brain/body rehabilitative benefits produced by this deep trance-like state that makes AVE so useful for so many conditions. The dissociative state can be first observed by noticing deep and diaphragmatic breathing. Hands and feet become warmer as arteries dilate. Skin colour will become pinker as blood flow increases throughout the face and body. Blood flow will increase in the brain as well. The person will experience feelings of profound relaxation and contentment as beneficial neurotransmitters are released into the brain. When in this deep state, the brain/body’s regenerative repair chemicals (parasympathetic hormones) and stabilizing neurotransmitters such as serotonin, endorphins and dopamine are released, which restore good brain function. AVE contributes to this restoration by providing a stress-break, increasing cerebral blood flow and encouraging impaired neuronal firing which allows the brain to return to normal function.
There are a number of things that are going on when you are using AVE:
1) Your EEG activity is being altered – As the AVE frequency changes, so does the frequency in the brain. For example, when an AVE unit is set to pulsate at 10 Hz alpha, the brain responds by producing more alpha which leads to a feeling of deep relaxation.
2) You are being dissociated – When using AVE, you get drawn into the present moment and let go of thoughts relating to your daily hassles, hectic schedules, paying bills, worries, threats or anxieties and stop mental “chatter.” Dissociation involves a “disconnection” of self from thoughts and body awareness, as is experienced during deep meditation. Dissociation begins in four to eight minutes from properly applied AVE.
3) Your limbic system is being stabilized – Your body is calmed, your breathing becomes rhythmic, your hands warm and your muscles relax.
4) A number of neurotransmitters are being produced – There is some evidence that people with depressed mood have low levels of serotonin and norepinephrine. AVE boosts brain levels of serotonin and norepinephrine to improve overall well-being.
5) Your cerebral blood flow (CBF) is being increased – CBF is associated with many forms of mental disorders, including anxiety, depression, attentional problems, behaviour disorders and impaired cognitive function. CBF tends to lower as we age and is correlated with cognitive decline. People experiencing depressed mood usually have lower levels of CBF in the left frontal and prefrontal lobes.
*Adapted from MindAlive.com
Click HERE to read more about the history of physiological mechanisms of AVE.